Opioids
The opioids domain of the Atlas of Healthcare Variation gives an overview on the dispensing of opioids by demographics and health district to identify areas of wide variation.
| Opioid atlas single map | Opioid atlas PHO analysis |
This update uses data from 2023. We have used primary health organisation (PHO) enrolment data as the denominator, replacing Stats NZ estimated population projections. This resulted in 3,678 people being excluded from the Atlas. This is less than 4 percent of the total count of 99,663 people dispensed a strong opioid in a year. There were no significant differences in the percent excluded due to not being enrolled by age, ethnicity or gender.
The methodology report has more information on the indicators, data sources, definitions and rationale we used to gather this data.
Atlas of Healthcare Variation: Methodology for opioids (PDF 570KB)
Atlas of Healthcare Variation: Methodology for opioids (DOCX 330KB)
Key findings
- The overall dispensing rate of both strong and weak opioids has increased significantly since 2019.
- Among older people aged 80 years or over, strong opioid dispensing has increased significantly since 2019 from 98.7 to 110.8 per 1,000 PHO-enrolled population, while weak opioid dispensing has continued to decline from 181.5 to 167.8 per 1,000 PHO-enrolled population.
- Overall rates of opioid dispensing are higher in people of European/Other ethnicity, women and people aged 80 years and over.
- Almost half of people dispensed a strong opioid had a ‘trigger event’ in a public hospital in the week prior, suggesting these prescriptions are generated in hospital.
- Oxycodone dispensing has increased significantly since 2019; rates varied about eight-fold between districts among people aged 80 years or over.
- Fentanyl dispensing increased significantly with age; rates varied 10-fold between districts.
Overview of opioid use
Opioids are a type of medicine used to treat pain. They are used a lot in hospital for patients to help ease pain but can also cause harm.
The Institute for Healthcare Improvement (IHI) classes opioids as one of four groups of medicines (along with anticoagulants, insulin and sedatives) that can cause harm to patients, even when used as intended.
Overview of opioid use
Opioid analgesia is the primary intervention for managing pain in hospital patients. Opioids are also considered effective treatment for severe pain in palliative care. [1] The National Institute for Health and Care Excellence (NICE) [1] recommends opioids should not be used for neuropathic pain without specialist assessment. There is limited evidence that opioids are effective for treating chronic non-cancer pain in the long term. [2]
Our analyses showed that strong opioid dispensing has increased over time, particularly among older adults. We also found that older adults were more likely to be dispensed strong opioids for six or more weeks. Long-term use of opioids should be used with extreme caution and the potential for serious adverse effects and complications be considered. [1,3]
Harm associated with opioid therapy include opioid tolerance, opioid-induced hyperalgesia, [4] iatrogenic addiction and dependency, drug diversion and aberrant drug-related behaviours. [1,5] In addition, a strong relationship between severe dependence on opioids and other substance use and mental health disorders has been observed.[6]
Health practitioners considering opioid therapy for chronic non-malignant pain are advised to conduct a thorough benefit-to-harm evaluation to determine whether opioids are the most appropriate option. This evaluation should include a detailed history, physical examination, and diagnostic assessment prior to initiating treatment, with ongoing review throughout the course of therapy.[1,7]
There is growing evidence showing that hospital encounters are a key trigger for opioid prescribing, especially in younger populations. [8] Our analysis also showed that nearly one in six young people who were dispensed a strong opioid went to hospital in the eight days prior to dispensing.
There is a concern whether even short-term opioid use can lead to prolonged exposure, especially if there is no clear plan to reassess the need for opioids or taper off them if necessary. [8] It underscores the need for targeted interventions at hospital discharge to ensure opioids are used safely, appropriately, and temporarily.
Pain management
Opioid analgesia is the primary intervention for managing pain in hospital patients. Opioids are also considered effective treatment for severe pain in palliative care. [1] The National Institute for Health and Care Excellence (NICE) [1] recommends opioids should not be used for neuropathic pain without specialist assessment. There is limited evidence that opioids are effective for treating chronic non-cancer pain in the long term. [2]
Dispensing has increased over time
Our analyses showed that strong opioid dispensing has increased over time, particularly among older adults. We also found that older adults were more likely to be dispensed strong opioids for six or more weeks. Long-term use of opioids should be used with extreme caution and the potential for serious adverse effects and complications be considered. [1,3]
Potential harm with opioid use
Harm associated with opioid therapy include opioid tolerance, opioid-induced hyperalgesia, [4] iatrogenic addiction and dependency, drug diversion and aberrant drug-related behaviours. [1,5] In addition, a strong relationship between severe dependence on opioids and other substance use and mental health disorders has been observed.[6]
Health practitioners considering opioid therapy for chronic non-malignant pain are advised to conduct a thorough benefit-to-harm evaluation to determine whether opioids are the most appropriate option. This evaluation should include a detailed history, physical examination, and diagnostic assessment prior to initiating treatment, with ongoing review throughout the course of therapy.[1,7]
Opioid prescribing in hospitals
There is growing evidence showing that hospital encounters are a key trigger for opioid prescribing, especially in younger populations. [8] Our analysis also showed that nearly one in six young people who were dispensed a strong opioid went to hospital in the eight days prior to dispensing.
Prolonged exposure to opioids
There is a concern whether even short-term opioid use can lead to prolonged exposure, especially if there is no clear plan to reassess the need for opioids or taper off them if necessary. [8] It underscores the need for targeted interventions at hospital discharge to ensure opioids are used safely, appropriately, and temporarily.
What the data tells us
Selected findings from the Atlas are summarised below. For all indicators and detailed commentary, see the Atlas dashboards, where you can search by age, ethnic group, year, and health district.
What the data tells us
- In 2023, excluding people receiving methadone for opioid substitution treatment,19.6 per 1,000 of the PHO-enrolled population was dispensed a strong opioid. This is a significant increase from 2019, when the rate was 15.5 per 1,000 people.
- Dispensing rates for strong opioids:
- varied significantly between districts; for example, rates ranged from 30.8 to 66.6 per 1,000 among those aged 65–79 years
- increased significantly by age; for example, about 110.8 per 1,000 people aged 80 years and over were dispensed a strong opioid, compared to younger age groups.
- varied by ethnic grouping; for example, among those aged 65-74 years Māori (53.4 per 1,000) had significantly higher rates than people belonging to other ethnic groupings (Pacific peoples 37.4; Asian 18.5 and European/Other 44.6 per 1,000)
- varied by gender; among people aged 80 years or over, women (122.2 per 1,000) were dispensed significantly more than men (95.9 per 1,000).
- Of the people receiving a strong opioid, 10.6 percent took the opioid for six or more weeks.
- In 2023, people aged 80 years and over were significantly more likely to be dispensed a strong opioid for six or more weeks than younger age groups.
A ‘weak’ opioid is classed as step 2 of WHO’s analgesic ladder. This includes tramadol, codeine and dihydrocodeine. These opioids are subsidised in New Zealand. Paracetamol with codeine is excluded because it contains a low dose of codeine.
- In 2023, about 105.1 per 1,000 of the PHO-enrolled population in New Zealand were dispensed a weak opioid, a significant increase from 2019 (103.0 per 1,000). Weak opioid use remains most common among older people aged 80 years and over (167.8 per 1,000 in 2023), despite a decline in rates for this age group since 2019 (181.5 per 1,000). Conversely, rates increased among the 25–64 age group, rising from 127.9 per 1,000 in 2019 to 132.0 per 1,000 in 2023.
- Ethnic differences exist; for example, among those 25–64 years, Māori (158.8 per 1,000) were significantly more likely to be prescribed weak opioids than other ethnic groups (Pacific peoples: 135.2; Asian: 85.3; European/Other:141.4 per 1,000).
- Tramadol was dispensed to fewer people overall than codeine or dihydrocodeine – 50.9 compared with 64.9 per 1,000. While tramadol dispensing is highest among those aged 25–64 and 65–79 years (67.8 and 67.3 per 1,000, respectively), dispensing of codeine or dihydrocodeine is highest among individuals aged 80 years and over (133.0 per 1,000).
- Tramadol dispensing in people aged 80 years and over has decreased from 49.9 per 1,000 in 2019 to 45.2 per 1,000 in 2023.As with strong opioids, women were dispensed significantly more weak opioids than men. For example, among those aged 80 years and over, women (179.0 per 1,000) were dispensed significantly more weak opioids than men (153.0 per 1,000).
- In 2023, about 12.9 per 1,000 of the PHO-enrolled population received morphine.
- Dispensing rates varied by district, for example, rate varied about three-fold between districts among those aged 80 years and over, ranging from 35.6 to 109.8 per 1,000 people.
- Of those dispensed a strong opioid in 2023, two-thirds (66.2 percent) received morphine.
- The number of people dispensed morphine has increased by about 13,665 people since 2019, from 10.5 to 12.9 per 1,000 people in 2023.
- One in ten people dispensed morphine continued taking it for six weeks or more. Among those aged 80 years or over who were dispensed morphine for six weeks or longer, more than nine out of ten belong to European/Other ethnicity.
- In 2023, about 7.2 per 1,000 of the PHO-enrolled population received oxycodone, a significant increase from 2019 (5.1 per 1,000).
- Rates varied by district; for example, among those aged 80 years or over, rates varied about eight-fold, ranging from 9.0–71.2 per 1,000 people.
- About 1 in 10 people dispensed oxycodone took it for six or more weeks.
- In 2023, about 1.4 per 1,000 of the PHO-enrolled population received fentanyl.
- Fentanyl dispensing significantly increased with age from 3.3 per 1,000 aged 65–79 years to 17.1 per 1,000 people aged 80 years and over.
- Rates varied by district; for example, among those aged 80 years or over, rates varied about 10-fold, ranging from 4.5-44.1 per 1,000 people.
- Of those given fentanyl, more than 20 percent took it for six or more weeks.
- Of every 10 people dispensed a strong opioid, nearly five attended a public hospital as an inpatient or outpatient in the week prior.
- Younger people were more likely to have a public hospital event prior to being dispensed a strong opioid compared with older people; 6 out of every 10 of those aged 0–24 years compared with 4 out of 10 of those aged 80 years and over.
- In 2023, among those aged 80 years or over, European/Other had the highest rates of strong opioid dispensing but had the lowest rates of public hospital events in the eight days prior to dispensing, compared to other ethnic groups.
The rate of strong opioid dispensing has increased since 2019
- In 2023, excluding people receiving methadone for opioid substitution treatment,19.6 per 1,000 of the PHO-enrolled population was dispensed a strong opioid. This is a significant increase from 2019, when the rate was 15.5 per 1,000 people.
- Dispensing rates for strong opioids:
- varied significantly between districts; for example, rates ranged from 30.8 to 66.6 per 1,000 among those aged 65–79 years
- increased significantly by age; for example, about 110.8 per 1,000 people aged 80 years and over were dispensed a strong opioid, compared to younger age groups.
- varied by ethnic grouping; for example, among those aged 65-74 years Māori (53.4 per 1,000) had significantly higher rates than people belonging to other ethnic groupings (Pacific peoples 37.4; Asian 18.5 and European/Other 44.6 per 1,000)
- varied by gender; among people aged 80 years or over, women (122.2 per 1,000) were dispensed significantly more than men (95.9 per 1,000).
- Of the people receiving a strong opioid, 10.6 percent took the opioid for six or more weeks.
- In 2023, people aged 80 years and over were significantly more likely to be dispensed a strong opioid for six or more weeks than younger age groups.
Dispensing of weak opioids varied by age
A ‘weak’ opioid is classed as step 2 of WHO’s analgesic ladder. This includes tramadol, codeine and dihydrocodeine. These opioids are subsidised in New Zealand. Paracetamol with codeine is excluded because it contains a low dose of codeine.
- In 2023, about 105.1 per 1,000 of the PHO-enrolled population in New Zealand were dispensed a weak opioid, a significant increase from 2019 (103.0 per 1,000). Weak opioid use remains most common among older people aged 80 years and over (167.8 per 1,000 in 2023), despite a decline in rates for this age group since 2019 (181.5 per 1,000). Conversely, rates increased among the 25–64 age group, rising from 127.9 per 1,000 in 2019 to 132.0 per 1,000 in 2023.
- Ethnic differences exist; for example, among those 25–64 years, Māori (158.8 per 1,000) were significantly more likely to be prescribed weak opioids than other ethnic groups (Pacific peoples: 135.2; Asian: 85.3; European/Other:141.4 per 1,000).
- Tramadol was dispensed to fewer people overall than codeine or dihydrocodeine – 50.9 compared with 64.9 per 1,000. While tramadol dispensing is highest among those aged 25–64 and 65–79 years (67.8 and 67.3 per 1,000, respectively), dispensing of codeine or dihydrocodeine is highest among individuals aged 80 years and over (133.0 per 1,000).
- Tramadol dispensing in people aged 80 years and over has decreased from 49.9 per 1,000 in 2019 to 45.2 per 1,000 in 2023.As with strong opioids, women were dispensed significantly more weak opioids than men. For example, among those aged 80 years and over, women (179.0 per 1,000) were dispensed significantly more weak opioids than men (153.0 per 1,000).
Morphine dispensing has increased since 2019
- In 2023, about 12.9 per 1,000 of the PHO-enrolled population received morphine.
- Dispensing rates varied by district, for example, rate varied about three-fold between districts among those aged 80 years and over, ranging from 35.6 to 109.8 per 1,000 people.
- Of those dispensed a strong opioid in 2023, two-thirds (66.2 percent) received morphine.
- The number of people dispensed morphine has increased by about 13,665 people since 2019, from 10.5 to 12.9 per 1,000 people in 2023.
- One in ten people dispensed morphine continued taking it for six weeks or more. Among those aged 80 years or over who were dispensed morphine for six weeks or longer, more than nine out of ten belong to European/Other ethnicity.
Oxycodone dispensing has increased significantly from 2019
- In 2023, about 7.2 per 1,000 of the PHO-enrolled population received oxycodone, a significant increase from 2019 (5.1 per 1,000).
- Rates varied by district; for example, among those aged 80 years or over, rates varied about eight-fold, ranging from 9.0–71.2 per 1,000 people.
- About 1 in 10 people dispensed oxycodone took it for six or more weeks.
Rates of fentanyl dispensing varied widely, particularly in those aged 80 and over
- In 2023, about 1.4 per 1,000 of the PHO-enrolled population received fentanyl.
- Fentanyl dispensing significantly increased with age from 3.3 per 1,000 aged 65–79 years to 17.1 per 1,000 people aged 80 years and over.
- Rates varied by district; for example, among those aged 80 years or over, rates varied about 10-fold, ranging from 4.5-44.1 per 1,000 people.
- Of those given fentanyl, more than 20 percent took it for six or more weeks.
Almost half of those dispensed a strong opioid had a public hospital ‘trigger event’
- Of every 10 people dispensed a strong opioid, nearly five attended a public hospital as an inpatient or outpatient in the week prior.
- Younger people were more likely to have a public hospital event prior to being dispensed a strong opioid compared with older people; 6 out of every 10 of those aged 0–24 years compared with 4 out of 10 of those aged 80 years and over.
- In 2023, among those aged 80 years or over, European/Other had the highest rates of strong opioid dispensing but had the lowest rates of public hospital events in the eight days prior to dispensing, compared to other ethnic groups.
Opioid dispensing for people aged 65 and over, by place of residence
In previous years we noticed a high rate of morphine dispensing among people aged 65 and over living in aged residential care (ARC). In contrast, the rate of morphine dispensing by people aged 65 and over not living in ARC is not increasing at the same rate.
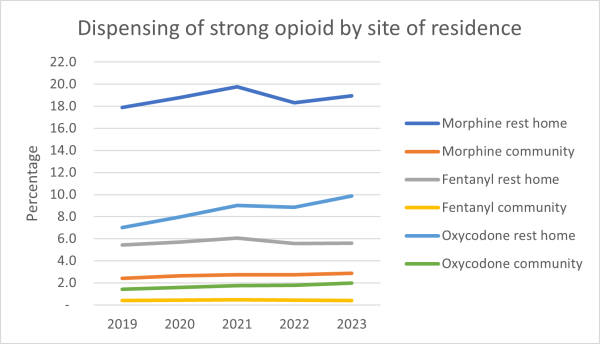
We explored what is causing the increase in aged residential care.
One of the most likely reasons for the difference could be the use of strong opioids for palliative care. Morphine is the recommended first-line opioid in palliative care.
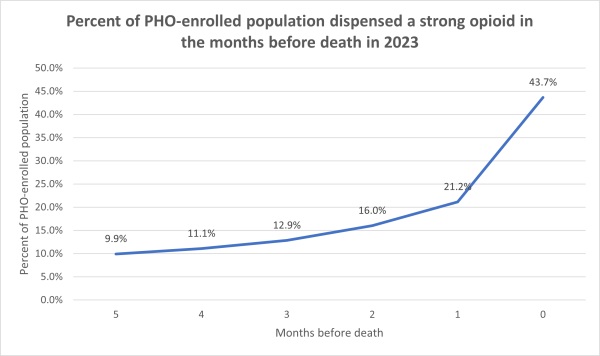
Dispensing strong opioids by type in the six months prior to a person’s death was also analysed. The graph below shows that strong opioid dispensing rates peak in the month of death, with 43.7 percent of people receiving a strong opioid in their last month of life.
Further analyses showed that 49.7 percent of aged residential care residents and 37.9 percent of people not living in aged residential care were dispensed a strong opioid in their last month of life.
Overall, in 2023, 55.9 percent of those in aged residential care and 43.0 percent of people not living in aged residential care were dispensed a strong opioid at some point in their last six of months of life.
About the data
Data for this Atlas domain was drawn from the Pharmaceutical Collection, which contains claim and payment information from community pharmacists for subsidised dispensing. This collection does not allow for analysis of patients’ condition or the effectiveness of dose provided. This means it’s not possible to assess the appropriateness or otherwise of prescribing.
Unsubsidised dispensing is not included in this analysis; nor does it indicate if people took the medicine.
This analysis focuses on the number of people dispensed opioids, not on the number of prescriptions of these medicines. We have used this approach because interpreting what the number of dispensed prescriptions might mean is complicated by differences in prescribing frequency, formulation and dose, and if the medicine is to be taken ‘as needed’ or at regular times.
We recommend further local analysis of the people receiving these medicines that accounts for these factors and the person’s clinical condition.
Atlas of Healthcare Variation: Methodology for opioids (PDF 570KB)
Atlas of Healthcare Variation: Methodology for opioids (DOCX 330KB)
Key findings from this update of the Opioids Atlas, which incorporates data through 2023, were discussed with clinicians to better understand potential drivers behind the increase in opioid dispensing. While strong opioids dispensing among older adults is high, this does not necessarily reflect inappropriate prescribing. Patterns appear to be a combination of clinical necessity (eg, comorbidities limiting alternatives), compassionate care priorities (comfort over long-term risk) and concerns about under-treating pain.
Our data shows that around 10 percent of strong opioids are dispensed for six or more weeks, and the rate has not substantially changed since 2019. However, high rates in people aged 80 and over and wide district variation (up to eight-fold variation in oxycodone dispensing) raise questions that warrant further exploration:
- Why do some districts have consistently lower or higher rates than the national mean? What impact might access to non-pharmacologic pain management have on these rates? What is the effect of a district’s access to specialist pain services on the use of opioids?
- How do districts with similar populations compare?
- How much are surgical wait times, ineligibility for surgery, weight gain and comorbidity contributing factors?
- How do opioid dispensing rates compare between regions with long surgical wait times versus those with better access to surgery?
- Is there a correlation between orthopaedic wait times and opioid dispensing rates?
- What are your district’s trends for opioid prescribing in aged residential care?
- What percentage of aged care residents on strong opioids were initiated during a hospital admission? How often are opioid dosage successfully tapered after discharge? What measures are in place at hospitals to limit opioid prescribing at discharge?
- What proportion of aged care residents remain on strong opioids for more than six weeks?
- How often do complaints about inadequate pain relief influence prescribing decisions? Does perceived ineffectiveness of paracetamol influence patient expectations and clinician prescribing? Does bulk availability and direct-to-consumer advertising of over-the-counter painkillers create a perception these products are ineffective, leading patients to request stronger medications?
- Why are there marked ethnic differences in the use of opioids? Is it the result of higher use in older people or might it reflect other differences, such as different cultural expressions of pain and different ways of coping with pain?
- What is the effect of access to palliative care services?
- What tools and skills do primary care providers have to manage chronic non-cancer pain?
- How can the impact of increased use of telehealth appointments, changes in prescriber workforce (eg, more international doctors, nurse practitioners, short-term locums) and 12-month prescribing be managed to ensure medication reviews are maintained?
- Are concerns about the “triple whammy” (NSAIDs + ACE inhibitors + diuretics) and renal risk in older people limiting non-opioid pain relief options? What guidance do regional health pathways provide for chronic pain management? Do repeat prescribing policies for analgesics and pain management need updating?
- What proportion of opioid prescriptions in aged residential care are for palliative or end-of-life care, chronic non-cancer pain, or changes in behaviour attributed to pain?
- How much is the increase in strong opioid, particularly oxycodone, dispensing related to palliative and end-of-life care?
- What other combinations of medicines are people receiving strong opioids for six or more weeks also receiving?
- How does the falls rate of older people in your district who are using opioids compare with the rate of those who are not? What is the extent of polypharmacy in older people who are using opioids?
- Might the removal of triplicate prescribing in 2021 have reduced barriers to opioid prescribing?
Data sources and method
Data for this Atlas domain was drawn from the Pharmaceutical Collection, which contains claim and payment information from community pharmacists for subsidised dispensing. This collection does not allow for analysis of patients’ condition or the effectiveness of dose provided. This means it’s not possible to assess the appropriateness or otherwise of prescribing.
Unsubsidised dispensing is not included in this analysis; nor does it indicate if people took the medicine.
This analysis focuses on the number of people dispensed opioids, not on the number of prescriptions of these medicines. We have used this approach because interpreting what the number of dispensed prescriptions might mean is complicated by differences in prescribing frequency, formulation and dose, and if the medicine is to be taken ‘as needed’ or at regular times.
We recommend further local analysis of the people receiving these medicines that accounts for these factors and the person’s clinical condition.
Atlas of Healthcare Variation: Methodology for opioids (PDF 570KB)
Atlas of Healthcare Variation: Methodology for opioids (DOCX 330KB)
What questions might the data prompt?
Key findings from this update of the Opioids Atlas, which incorporates data through 2023, were discussed with clinicians to better understand potential drivers behind the increase in opioid dispensing. While strong opioids dispensing among older adults is high, this does not necessarily reflect inappropriate prescribing. Patterns appear to be a combination of clinical necessity (eg, comorbidities limiting alternatives), compassionate care priorities (comfort over long-term risk) and concerns about under-treating pain.
Our data shows that around 10 percent of strong opioids are dispensed for six or more weeks, and the rate has not substantially changed since 2019. However, high rates in people aged 80 and over and wide district variation (up to eight-fold variation in oxycodone dispensing) raise questions that warrant further exploration:
- Why do some districts have consistently lower or higher rates than the national mean? What impact might access to non-pharmacologic pain management have on these rates? What is the effect of a district’s access to specialist pain services on the use of opioids?
- How do districts with similar populations compare?
- How much are surgical wait times, ineligibility for surgery, weight gain and comorbidity contributing factors?
- How do opioid dispensing rates compare between regions with long surgical wait times versus those with better access to surgery?
- Is there a correlation between orthopaedic wait times and opioid dispensing rates?
- What are your district’s trends for opioid prescribing in aged residential care?
- What percentage of aged care residents on strong opioids were initiated during a hospital admission? How often are opioid dosage successfully tapered after discharge? What measures are in place at hospitals to limit opioid prescribing at discharge?
- What proportion of aged care residents remain on strong opioids for more than six weeks?
- How often do complaints about inadequate pain relief influence prescribing decisions? Does perceived ineffectiveness of paracetamol influence patient expectations and clinician prescribing? Does bulk availability and direct-to-consumer advertising of over-the-counter painkillers create a perception these products are ineffective, leading patients to request stronger medications?
- Why are there marked ethnic differences in the use of opioids? Is it the result of higher use in older people or might it reflect other differences, such as different cultural expressions of pain and different ways of coping with pain?
- What is the effect of access to palliative care services?
- What tools and skills do primary care providers have to manage chronic non-cancer pain?
- How can the impact of increased use of telehealth appointments, changes in prescriber workforce (eg, more international doctors, nurse practitioners, short-term locums) and 12-month prescribing be managed to ensure medication reviews are maintained?
- Are concerns about the “triple whammy” (NSAIDs + ACE inhibitors + diuretics) and renal risk in older people limiting non-opioid pain relief options? What guidance do regional health pathways provide for chronic pain management? Do repeat prescribing policies for analgesics and pain management need updating?
- What proportion of opioid prescriptions in aged residential care are for palliative or end-of-life care, chronic non-cancer pain, or changes in behaviour attributed to pain?
- How much is the increase in strong opioid, particularly oxycodone, dispensing related to palliative and end-of-life care?
- What other combinations of medicines are people receiving strong opioids for six or more weeks also receiving?
- How does the falls rate of older people in your district who are using opioids compare with the rate of those who are not? What is the extent of polypharmacy in older people who are using opioids?
- Might the removal of triplicate prescribing in 2021 have reduced barriers to opioid prescribing?
Resources
This short report summarises rural–urban differences in opioid dispensing, examining patterns in both strong and weak opioids across New Zealand.
Rural-urban variation
This short report summarises rural–urban differences in opioid dispensing, examining patterns in both strong and weak opioids across New Zealand.
Further reading
- Neuropathic pain in adults: pharmacological management in non-specialist settings. (nice.org.uk)
- Efficacy of interventions to reduce long term opioid treatment for chronic non-cancer pain: systematic review and meta-analysis (bmj.com)
- Clinical Audit - Reviewing patients using opioid medicines long-term for non-cancer pain (bpac.org.nz)
- Lack of correlation between opioid dose adjustment and pain score change in a group of chronic pain patients. (pubmed.ncbi.nlm.nih.gov)
- Problems and concerns of patients receiving chronic opioid therapy for chronic non-cancer pain (pubmed.ncbi.nlm.nih.gov)
- Mental disorder and opioid overdose: a systematic review (pubmed.ncbi.nlm.nih.gov)
- Comprehensive, Evidence-Based, Consensus Guidelines for Prescription of Opioids for Chronic Non-Cancer Pain (pubmed.ncbi.nlm.gov)
- Global perspectives on opioid use: shifting the conversation from deprescribing to quality use of medicines (qualitysafety.bmj.com)
- Revisiting opioid use in New Zealand: how does your prescribing compare? (bpac.org.nz)
- Acute Pain Management: Scientific Evidence 5th edition (anzca.edu.au)
- Helping patients cope with chronic non-malignant pain: it’s not about opioids (bpac.org.nz)
- Identifying and managing addiction to opioids (bpac.org.nz)
- Upfront: “A disaster in the making”: it’s time to take action against misuse of oxycodone (bpac.org.nz)
- Oxycodone Update (bpac.org.nz)
- Revisiting opioid use in New Zealand: how does your prescribing compare? (bpac.org.nz)
- Clinical Audit - Reviewing patients using opioid medicines long-term for non-cancer pain (bpac.org.nz)
- Deprescribing opioids (bpac.org.nz)
- Adverse events associated with medium‐ and long‐term use of opioids for chronic non‐cancer pain: an overview of Cochrane Reviews (cochranelibrary.com)
- Patterns of opioid use in New Zealand older adults, 2007–2018 (onlinelibrary.wiley.com)
- Persistent opioid use and opioid-related harm after hospital admissions for surgery and trauma in New Zealand: a population-based cohort study (bmjopen.bmj.com)
- Persistent opioid use after hospital admission from surgery in New Zealand: A population-based study (journals.lww.com)
- Outcomes related to new persistent opioid use after surgery or trauma: a population-based cohort study (journals.lww.com)
- Opioid medicines overview (healthify.nz)
- Safe access to opioids: Engagement summary (health.govt.nz)
- Neuropathic pain in adults: pharmacological management in non-specialist settings (nice.org.uk)
- Chronic pain (primary and secondary) in over 16s: assessment of all chronic pain and management of chronic primary pain (nice.org.uk)
- Neuropathic pain in adults: pharmacological management in non-specialist settings (nice.org.uk)
- Management of opioid dependence (researchreview.co.nz)
- Prescribing drugs of dependence in general practice, Part C2 (racgp.org.au)
- New Zealand practice guidelines for opioid substitution treatment (health.govt.nz)
- SIGN 136. Management of chronic pain. A national clinical guideline (sign.ac.uk)
- Opioid Analgesic Stewardship acute pain clinical standard (safetyandquality.gov.au)
References
- Neuropathic pain in adults: pharmacological management in non-specialist settings. (nice.org.uk)
- Efficacy of interventions to reduce long term opioid treatment for chronic non-cancer pain: systematic review and meta-analysis (bmj.com)
- Clinical Audit - Reviewing patients using opioid medicines long-term for non-cancer pain (bpac.org.nz)
- Lack of correlation between opioid dose adjustment and pain score change in a group of chronic pain patients. (pubmed.ncbi.nlm.nih.gov)
- Problems and concerns of patients receiving chronic opioid therapy for chronic non-cancer pain (pubmed.ncbi.nlm.nih.gov)
- Mental disorder and opioid overdose: a systematic review (pubmed.ncbi.nlm.nih.gov)
- Comprehensive, Evidence-Based, Consensus Guidelines for Prescription of Opioids for Chronic Non-Cancer Pain (pubmed.ncbi.nlm.gov)
- Global perspectives on opioid use: shifting the conversation from deprescribing to quality use of medicines (qualitysafety.bmj.com)
- Revisiting opioid use in New Zealand: how does your prescribing compare? (bpac.org.nz)
Recommended reading
- Acute Pain Management: Scientific Evidence 5th edition (anzca.edu.au)
- Helping patients cope with chronic non-malignant pain: it’s not about opioids (bpac.org.nz)
- Identifying and managing addiction to opioids (bpac.org.nz)
- Upfront: “A disaster in the making”: it’s time to take action against misuse of oxycodone (bpac.org.nz)
- Oxycodone Update (bpac.org.nz)
- Revisiting opioid use in New Zealand: how does your prescribing compare? (bpac.org.nz)
- Clinical Audit - Reviewing patients using opioid medicines long-term for non-cancer pain (bpac.org.nz)
- Deprescribing opioids (bpac.org.nz)
- Adverse events associated with medium‐ and long‐term use of opioids for chronic non‐cancer pain: an overview of Cochrane Reviews (cochranelibrary.com)
- Patterns of opioid use in New Zealand older adults, 2007–2018 (onlinelibrary.wiley.com)
- Persistent opioid use and opioid-related harm after hospital admissions for surgery and trauma in New Zealand: a population-based cohort study (bmjopen.bmj.com)
- Persistent opioid use after hospital admission from surgery in New Zealand: A population-based study (journals.lww.com)
- Outcomes related to new persistent opioid use after surgery or trauma: a population-based cohort study (journals.lww.com)
- Opioid medicines overview (healthify.nz)
- Safe access to opioids: Engagement summary (health.govt.nz)
- Neuropathic pain in adults: pharmacological management in non-specialist settings (nice.org.uk)
- Chronic pain (primary and secondary) in over 16s: assessment of all chronic pain and management of chronic primary pain (nice.org.uk)
- Neuropathic pain in adults: pharmacological management in non-specialist settings (nice.org.uk)
- Management of opioid dependence (researchreview.co.nz)
- Prescribing drugs of dependence in general practice, Part C2 (racgp.org.au)
- New Zealand practice guidelines for opioid substitution treatment (health.govt.nz)
- SIGN 136. Management of chronic pain. A national clinical guideline (sign.ac.uk)
- Opioid Analgesic Stewardship acute pain clinical standard (safetyandquality.gov.au)