Polypharmacy in people aged 65 and over
The goal of this Atlas domain is to identify whether there is significant variation in the dispensing rates of long-term medications among people aged 65 and over, that may highlight areas that warrant further local investigation.
Overview
Polypharmacy refers to the concurrent use of multiple medicines by a person. It can be beneficial (appropriate polypharmacy) or harmful (inappropriate polypharmacy).[1]
- Appropriate polypharmacy has been described as medications that are clinically justified.
- Inappropriate polypharmacy is the prescribing of medications that are unnecessary, unhelpful or unwanted or have unacceptable side effects or risks. One way to define inappropriate polypharmacy is to look at the number of medicines (five or more medicines is often quoted).[2]
Polypharmacy is associated with:
- people not taking medicines as prescribed
- significant costs to patients and health services
- adverse drug events and drug interactions that can result in poor health outcomes, such as falls, cognitive impairment, frailty, depression and lower quality of life.
The risk of adverse drug events increases with the number of medications taken, with an inflexion point at five medications where the risk of side effects accelerates. Polypharmacy is consistently associated with higher rates of medication-related harm, including drug interactions, hospitalisations and poorer health outcomes [3,4].
Polypharmacy is more likely to be appropriate in those aged 65 to 74 while inappropriate polypharmacy is more likely to occur in those aged 85 and over. Hence a focus on the 85 years and over age group may be most appropriate, where the doses used may be as important as the number of medicines.
Key methodological changes in this update
- This update uses primary health organisation (PHO) enrolled population aged 65 years and over as the denominator, replacing Stats NZ estimated population projections. As a result, a small proportion of people were excluded from analysis in the interests of having a more tightly defined denominator. For example, approximately 3,600 people were excluded from Indicator 1 (people aged 65 years and over dispensed five or more unique long-term medicines). This represents less than 1 percent of those aged 65 years and over who were dispensed five or more unique medications.
- A key change was made to the numerator calculation, to make the approach more consistent with other Atlas methods.
Impact of these changes are listed in the table below:
| Indicator | Method change | Impact of method changes |
|
1. People aged 65 years and over dispensed five or more unique long-term medicines |
Previously, the numerator was calculated as the quarterly sum of individuals who received medications in a given quarter and had also been dispensed the same medications in the preceding quarter. This was averaged across four quarters. This update counts the distinct number of individuals who received the same medications in two consecutive quarters in a year. Therefore, current figures are not directly comparable with those from the previous update. This change was made to better capture those who may not receive five or more medicines consistently throughout the entire year, and to ensure consistency with other Atlas indicators, where we report medication use on an annual basis rather than as an average. |
The dispensing rate of 5+ medications increased from 32.1% in 2019 to 44.4% with the method change. Since 2019, this has increased to 46.5% in 2023. |
| 2. People aged 65 years and over dispensed five, six or seven unique long-term medicines | The rate in 2019 has increased from 19.2% to 33.1% with the method change. Rates have remained steady since. | |
| 3. People aged 65 years and over dispensed eight, nine or ten unique long-term medicines | In the previous version the rate was 8.9% in 2019, this has increased to 16.5% with the method change. The rate in 2023 was 17.9%. | |
| 4. People aged 65 years and over dispensed 11 or more unique long-term medicines | Reported at 4.0% in 2019, this increased to 6.8% with the method change, and to 8.1% in 2023. | |
| 5. People aged 65 years and over who received the ‘triple whammy’ | No change to numerator calculation. | The reported rate in 2019 was previously 3.2%, it is now 3.4%. In 2023, the rate has reduced to 2.7%. |
| 6. PHO-enrolled population aged 65 years and over who received an antipsychotic during the year | The earlier method used a quarterly average of individuals dispensed medications. This update instead counts the distinct number of individuals who received medications in at least one quarter of the calendar year. This is consistent with our usual methodology. | Antipsychotic use was 2.9% in 2019, rising to 4.3% with the method change. In 2023, the rate was 4.9%. |
| 7. PHO-enrolled population aged 65 years and over who received a benzodiazepine or zopiclone | The rate reported in 2019 was 10.4%, increasing to 17.1% with the method change. The rate in 2023 was reduced slightly to 16.2%. | |
| 8. People aged 65 years and over who received both a benzodiazepine or zopiclone and an antipsychotic in the same quarter during the calendar year | Reported rates were between 1–1.3% from 2012 to 2019, increasing slightly to 1.8% with the method change. Rates have remained unchanged since. |
The methodology report has more information on the indicators, data sources, definitions and rationale we used to gather this data.
Atlas of Healthcare Variation: Methodology for polypharmacy (PDF 535KB)
Atlas of Healthcare Variation: Methodology for polypharmacy (DOCX 330KB)
What the data tells us
Selected findings from the Atlas are summarised below. For all indicators and detailed commentary, see the Atlas dashboards, where you can search by age, ethnic group, year, and health district.
What the data tells us
- 46.5 percent of people aged 65 years and over received five or more long-term medicines (defined as five or more of the same chemicals dispensed over two consecutive quarters). 33.3 percent of people received 5 to 7 long-term medications, 17.9 percent of people received 8 to 10 long-term medications and 8.1 percent of people received 11 or more long-term medications (noting that these groups are not mutually exclusive).
- The rate of people dispensed five or more long-term medicines increased significantly with age, from 36.7 percent among those aged 65–74 years to 69.2 percent among those aged 85 years and over. The rate of older people receiving 11 or more long-term medicines increased sharply with age: 13.9 percent of those aged 85 years and over received 11 or more medicines, nearly 2.5 times the rate of those aged 65–74 years (5.7 percent).
- Rates varied significantly by ethnic group. Māori and Pacific peoples received more medicines at a younger age compared with those identifying as Asian or European/Other. For example, among the younger cohort (aged 65–74 years), Pacific peoples (10.9 percent) and Māori (9.1 percent) were more likely than other ethnic groups – Asian (5.7 percent) and European/Other (5.0 percent) – to receive 11 or more medications over two consecutive quarters in 2023.
- Rates also varied by district, ranging from 49.7 percent to 60.4 percent among those aged 75–84 years.
Table 1 shows the percentage and count by age group and ethnic group of those dispensed five or more long-term medicines.
| Ethnic Group | Age group (years) | |||||
|---|---|---|---|---|---|---|
| 65–74 | 75–84 | 85+ | ||||
| % | count | % | count | % | count | |
| Māori | 47.2 | 39,497 | 63.4 | 8,831 | 69.6 | 1,971 |
| Pacific peoples | 55.2 | 18,277 | 65.5 | 4,910 | 64.0 | 1049 |
| Asian | 35.7 | 47,063 | 55.5 | 9,961 | 64.9 | 3,394 |
| European/Other | 34.7 | 353,581 | 54.5 | 125,523 | 69.6 | 56,732 |
| Age % | ||||
| 65–74 | 75–84 | 85 and over | Total | |
| Dispensed five or more long-term medicines | 36.7 | 55.3 | 69.2 | 46.5 |
| 5–7 long-term medicines | 27.5 | 38.8 | 46.7 | 33.3 |
| 8–10 long-term medicines | 12.8 | 22.1 | 30.9 | 17.9 |
| 11 or more long-term medicines | 5.7 | 10.3 | 13.9 | 8.1 |
| Note: these groups are not mutually exclusive. | ||||
| Long-term medicines dispensed (%) | ||||
| Ethnic group | Five or more | 5–7 | 8–10 | 11 or more |
| Māori | 52.3 | 35.5 | 21.9 | 10.5 |
| Pacific peoples | 58.5 | 37.8 | 25.5 | 12.2 |
| Asian | 42.9 | 29.6 | 16.6 | 7.9 |
| European/Other | 45.8 | 33.4 | 17.3 | 7.7 |
The triple whammy is the combination of an angiotensin converting enzyme (ACE) inhibitor/angiotensin receptor blocker (ARB), a diuretic and a non-steroidal anti-inflammatory drug (NSAID).
Medsafe notes an increased risk of acute kidney injury with this combination, especially in people with risk factors for renal failure and in older adults.[5] The combination should be avoided if possible.
- Of those aged 65 years and over, 2.7 percent were dispensed the triple whammy within the same 90-day period. This equates to 21,750 people in 2023. The rate has significantly decreased from 2019 (3.4 percent), which is about 3,500 fewer people.
- Rates varied significantly by ethnic grouping; for example, among those aged 65–74 years Māori (3.6 percent) and Pacific peoples (3.4 percent) were significantly higher than Asian (1.8 percent) or European/Other (2.7 percent). Rates were lowest among older people aged 85 years and over across all ethnic groups.
- Females were more likely to be dispensed triple whammy in the same 90-day period when compared to males. This pattern is consistent across all age groups.
- Rates also varied significantly by district; for example, among those aged 75–84 years, rates varied by more than 2.5-fold, ranging from 2.1 to 5.5 percent.
- This indicator does not include those who bought an NSAID over the counter or had a prescription in a previous period.
In older people, certain classes of medicines carry a substantially higher risk of adverse effects. Two examples presented in this Atlas domain are antipsychotics and a benzodiazepine or zopiclone. Common adverse effects include impaired functional ability, agitation, confusion, blurred vision, urinary retention, constipation, postural hypotension and falls. These increase if both classes of medicine are taken together. This indicator cannot assess inappropriate use of these medicines; however, high rates of prescribing may indicate misuse or overuse.
- The dispensing of psychotropic agents increases with age. For example, 13.5 percent of 65–74 year olds received a benzodiazepine or zopiclone in 2023 compared with 25.8 percent of those aged 85 and over.
- Benzodiazepine or zopiclone is more commonly used (16.2 percent) than an antipsychotic (4.9 percent) and, since 2019, dispensing rates of both classes have remained steady.
- Antipsychotic dispensing rates are significantly higher for Māori across all age groups compared with other ethnicities. Rates also varied by district; for example, among those aged 85 years and over, rates ranged more than twofold – from 8.1 percent to 16.9 percent.
- Benzodiazepine or zopiclone dispensing rates are significantly higher among European/Other populations at all ages. Among those aged 85 years and over, 26.3 percent of European/Other individuals were dispensed these medicines, compared to 19.6 percent of Asian, 18.3 percent of Māori, and 9.4 percent of Pacific peoples. Rates also varied significantly by district.
- Females were more likely to be dispensed benzodiazepine or zopiclone when compared to males. This pattern is consistent across all age groups.
- The rate of combined use of antipsychotics and benzodiazepine or zopiclone was relatively low (2.1 percent) but increased with age—from 1.3 percent among those aged 65–74 years to 6.0 percent among those aged 85 years and over.
Psychotropic medication increases the risk of falling [6] and there is evidence that reducing psychotropic medication can result in no or limited worsening of key outcomes such as sleep quality or behavioural problems.[6, 7] The most recent Australian and New Zealand Hip Fracture Registry (ANZHFR report) shows that in 2023, the rate remains high at around 22 per 1,000 in this age group, confirming that hip fractures continue to be a major burden among older adults [8].
Our analysis showed significant differences in the dispensing of multiple medications between people who lived in aged residential care (ARC) and those who didn’t, in 2023:
- 86 percent of people living in aged residential care were dispensed five or more medications in two consecutive quarters, compared to 45 percent of people not living in aged residential care
- 28 percent of ARC residents were dispensed 11 or more medications, compared to 7.1 percent of people not living in aged residential care.
For age-specific rates, please refer to Figure 1.
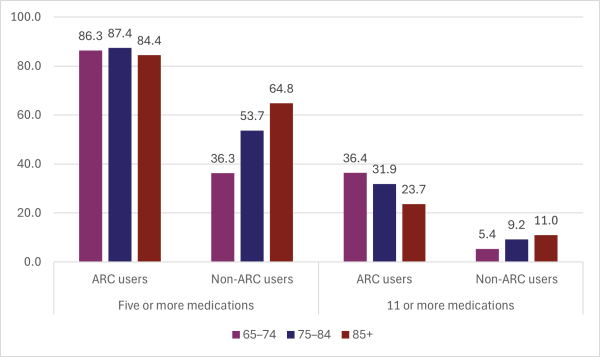
Figure 1: Polypharmacy rates in people living in aged residential care and those not living in aged residential care, by age group (percent), 2023
It is pleasing to see the reduction in ‘triple whammy’ dispensing since 2019. Key findings from this update include high dispensing rates of 11 or more medications – particularly among those aged 85 years and over – and notable differences between people living in aged residential care and those who are not. These findings warrant further investigation.
- Why do we see such high rates of polypharmacy (11+ medications) among people in aged residential care? How much of this is driven by guideline-based prescribing versus clinical complexity and multimorbidity?
- How do similar districts compare?
- Why are Māori and Pacific peoples receiving more medications at younger ages? Could earlier onset of multiple comorbidities in some groups drive multiple medications from the outset?
- Why are greater proportions of European/Other people aged 65 years and over dispensed a benzodiazepine or zopiclone than Māori or Pacific peoples?
- How often are medications reviewed or deprescribed, particularly after hospital discharge or in aged care settings?
What tools or frameworks can support safe deprescribing in ARC settings? - Are there any strategies for practitioners to minimise harm from deprescribing (eg, decompensation in heart failure) while also avoiding harm from overprescribing?
- What role might secondary clinicians have in influencing prescribing patterns in their community?
Overall, the rate of dispensing of five or more long-term medicines has increased since 2019. Rates are higher for Pacific peoples, Māori and those aged 85 and over
- 46.5 percent of people aged 65 years and over received five or more long-term medicines (defined as five or more of the same chemicals dispensed over two consecutive quarters). 33.3 percent of people received 5 to 7 long-term medications, 17.9 percent of people received 8 to 10 long-term medications and 8.1 percent of people received 11 or more long-term medications (noting that these groups are not mutually exclusive).
- The rate of people dispensed five or more long-term medicines increased significantly with age, from 36.7 percent among those aged 65–74 years to 69.2 percent among those aged 85 years and over. The rate of older people receiving 11 or more long-term medicines increased sharply with age: 13.9 percent of those aged 85 years and over received 11 or more medicines, nearly 2.5 times the rate of those aged 65–74 years (5.7 percent).
- Rates varied significantly by ethnic group. Māori and Pacific peoples received more medicines at a younger age compared with those identifying as Asian or European/Other. For example, among the younger cohort (aged 65–74 years), Pacific peoples (10.9 percent) and Māori (9.1 percent) were more likely than other ethnic groups – Asian (5.7 percent) and European/Other (5.0 percent) – to receive 11 or more medications over two consecutive quarters in 2023.
- Rates also varied by district, ranging from 49.7 percent to 60.4 percent among those aged 75–84 years.
Table 1 shows the percentage and count by age group and ethnic group of those dispensed five or more long-term medicines.
| Ethnic Group | Age group (years) | |||||
|---|---|---|---|---|---|---|
| 65–74 | 75–84 | 85+ | ||||
| % | count | % | count | % | count | |
| Māori | 47.2 | 39,497 | 63.4 | 8,831 | 69.6 | 1,971 |
| Pacific peoples | 55.2 | 18,277 | 65.5 | 4,910 | 64.0 | 1049 |
| Asian | 35.7 | 47,063 | 55.5 | 9,961 | 64.9 | 3,394 |
| European/Other | 34.7 | 353,581 | 54.5 | 125,523 | 69.6 | 56,732 |
| Age % | ||||
| 65–74 | 75–84 | 85 and over | Total | |
| Dispensed five or more long-term medicines | 36.7 | 55.3 | 69.2 | 46.5 |
| 5–7 long-term medicines | 27.5 | 38.8 | 46.7 | 33.3 |
| 8–10 long-term medicines | 12.8 | 22.1 | 30.9 | 17.9 |
| 11 or more long-term medicines | 5.7 | 10.3 | 13.9 | 8.1 |
| Note: these groups are not mutually exclusive. | ||||
| Long-term medicines dispensed (%) | ||||
| Ethnic group | Five or more | 5–7 | 8–10 | 11 or more |
| Māori | 52.3 | 35.5 | 21.9 | 10.5 |
| Pacific peoples | 58.5 | 37.8 | 25.5 | 12.2 |
| Asian | 42.9 | 29.6 | 16.6 | 7.9 |
| European/Other | 45.8 | 33.4 | 17.3 | 7.7 |
‘Triple whammy’ dispensing in people aged 65 years and over has significantly decreased since 2019 – about 3,500 fewer individuals.
The triple whammy is the combination of an angiotensin converting enzyme (ACE) inhibitor/angiotensin receptor blocker (ARB), a diuretic and a non-steroidal anti-inflammatory drug (NSAID).
Medsafe notes an increased risk of acute kidney injury with this combination, especially in people with risk factors for renal failure and in older adults.[5] The combination should be avoided if possible.
- Of those aged 65 years and over, 2.7 percent were dispensed the triple whammy within the same 90-day period. This equates to 21,750 people in 2023. The rate has significantly decreased from 2019 (3.4 percent), which is about 3,500 fewer people.
- Rates varied significantly by ethnic grouping; for example, among those aged 65–74 years Māori (3.6 percent) and Pacific peoples (3.4 percent) were significantly higher than Asian (1.8 percent) or European/Other (2.7 percent). Rates were lowest among older people aged 85 years and over across all ethnic groups.
- Females were more likely to be dispensed triple whammy in the same 90-day period when compared to males. This pattern is consistent across all age groups.
- Rates also varied significantly by district; for example, among those aged 75–84 years, rates varied by more than 2.5-fold, ranging from 2.1 to 5.5 percent.
- This indicator does not include those who bought an NSAID over the counter or had a prescription in a previous period.
Antipsychotic and benzodiazepine or zopiclone dispensing increases significantly with age
In older people, certain classes of medicines carry a substantially higher risk of adverse effects. Two examples presented in this Atlas domain are antipsychotics and a benzodiazepine or zopiclone. Common adverse effects include impaired functional ability, agitation, confusion, blurred vision, urinary retention, constipation, postural hypotension and falls. These increase if both classes of medicine are taken together. This indicator cannot assess inappropriate use of these medicines; however, high rates of prescribing may indicate misuse or overuse.
- The dispensing of psychotropic agents increases with age. For example, 13.5 percent of 65–74 year olds received a benzodiazepine or zopiclone in 2023 compared with 25.8 percent of those aged 85 and over.
- Benzodiazepine or zopiclone is more commonly used (16.2 percent) than an antipsychotic (4.9 percent) and, since 2019, dispensing rates of both classes have remained steady.
- Antipsychotic dispensing rates are significantly higher for Māori across all age groups compared with other ethnicities. Rates also varied by district; for example, among those aged 85 years and over, rates ranged more than twofold – from 8.1 percent to 16.9 percent.
- Benzodiazepine or zopiclone dispensing rates are significantly higher among European/Other populations at all ages. Among those aged 85 years and over, 26.3 percent of European/Other individuals were dispensed these medicines, compared to 19.6 percent of Asian, 18.3 percent of Māori, and 9.4 percent of Pacific peoples. Rates also varied significantly by district.
- Females were more likely to be dispensed benzodiazepine or zopiclone when compared to males. This pattern is consistent across all age groups.
- The rate of combined use of antipsychotics and benzodiazepine or zopiclone was relatively low (2.1 percent) but increased with age—from 1.3 percent among those aged 65–74 years to 6.0 percent among those aged 85 years and over.
Psychotropic medication increases the risk of falling [6] and there is evidence that reducing psychotropic medication can result in no or limited worsening of key outcomes such as sleep quality or behavioural problems.[6, 7] The most recent Australian and New Zealand Hip Fracture Registry (ANZHFR report) shows that in 2023, the rate remains high at around 22 per 1,000 in this age group, confirming that hip fractures continue to be a major burden among older adults [8].
Polypharmacy in Aged Residential Care (ARC)
Our analysis showed significant differences in the dispensing of multiple medications between people who lived in aged residential care (ARC) and those who didn’t, in 2023:
- 86 percent of people living in aged residential care were dispensed five or more medications in two consecutive quarters, compared to 45 percent of people not living in aged residential care
- 28 percent of ARC residents were dispensed 11 or more medications, compared to 7.1 percent of people not living in aged residential care.
For age-specific rates, please refer to Figure 1.
Figure 1: Polypharmacy rates in people living in aged residential care and those not living in aged residential care, by age group (percent), 2023
What questions might the data prompt?
It is pleasing to see the reduction in ‘triple whammy’ dispensing since 2019. Key findings from this update include high dispensing rates of 11 or more medications – particularly among those aged 85 years and over – and notable differences between people living in aged residential care and those who are not. These findings warrant further investigation.
- Why do we see such high rates of polypharmacy (11+ medications) among people in aged residential care? How much of this is driven by guideline-based prescribing versus clinical complexity and multimorbidity?
- How do similar districts compare?
- Why are Māori and Pacific peoples receiving more medications at younger ages? Could earlier onset of multiple comorbidities in some groups drive multiple medications from the outset?
- Why are greater proportions of European/Other people aged 65 years and over dispensed a benzodiazepine or zopiclone than Māori or Pacific peoples?
- How often are medications reviewed or deprescribed, particularly after hospital discharge or in aged care settings?
What tools or frameworks can support safe deprescribing in ARC settings? - Are there any strategies for practitioners to minimise harm from deprescribing (eg, decompensation in heart failure) while also avoiding harm from overprescribing?
- What role might secondary clinicians have in influencing prescribing patterns in their community?
Further reading
- Polypharmacy audit: Monitoring and reducing problematic prescribing (bpac.org.nz)
- Polypharmacy in primary care: Managing a clinical conundrum (bpac.org.nz)
- Managing medicines in older people (bpac.org.nz)
- Deprescribing.org
- Video: ‘The Geriatrician’s Scalpel: Pharmacological Debridement’ (youtube.com)
- Minimizing Inappropriate Medications in Older Populations: A 10-step Conceptual Framework (pubmed.ncbi.nlm.nih.gov)
- Managing the risks of polypharmacy in chronic disease (pharmac.govt.nz)
- Medication safety in polypharmacy: technical report (who.int)
- The triple whammy of (ACE/ARB) + (diuretic) + (NSAID) is a dangerous trio (gooodfellowunit.org)
- Interventions to improve the appropriate use of polypharmacy for older people (cochranelibrary.com)
- Don’t use antipsychotics routinely to treat agitation and aggression in people with dementia (bmj.com)
- Assessing medication burden and polypharmacy: finding the perfect measure (tandfonline.com)
- The rising tide of polypharmacy and drug-drug interactions: population database analysis 1995–2010 (link.springer.com)
- Drug interactions affecting kidney function: Beware of health threats from triple whammy (link.springer.com)
- Variation in benzodiazepine and antipsychotic use in people aged 65 years and over in New Zealand (pubmed.ncbi.nlm.nih.gov)
- A whole of population retrospective observational study on the rates of polypharmacy in New Zealand 2014 to 2018 Polypharmacy in New Zealand: What is the current status? (onlinelibrary.wiley.com)
- Preventing acute kidney injury: assessing awareness to temporarily discontinue 'at-risk' medicines during acute illness in a New Zealand cohort (pubmed.ncbi.nlm.nih.gov)
More information on medication review and managing polypharmacy
- Polypharmacy audit: Monitoring and reducing problematic prescribing (bpac.org.nz)
- Polypharmacy in primary care: Managing a clinical conundrum (bpac.org.nz)
- Managing medicines in older people (bpac.org.nz)
- Deprescribing.org
- Video: ‘The Geriatrician’s Scalpel: Pharmacological Debridement’ (youtube.com)
- Minimizing Inappropriate Medications in Older Populations: A 10-step Conceptual Framework (pubmed.ncbi.nlm.nih.gov)
- Managing the risks of polypharmacy in chronic disease (pharmac.govt.nz)
- Medication safety in polypharmacy: technical report (who.int)
Recommended reading
- The triple whammy of (ACE/ARB) + (diuretic) + (NSAID) is a dangerous trio (gooodfellowunit.org)
- Interventions to improve the appropriate use of polypharmacy for older people (cochranelibrary.com)
- Don’t use antipsychotics routinely to treat agitation and aggression in people with dementia (bmj.com)
- Assessing medication burden and polypharmacy: finding the perfect measure (tandfonline.com)
- The rising tide of polypharmacy and drug-drug interactions: population database analysis 1995–2010 (link.springer.com)
- Drug interactions affecting kidney function: Beware of health threats from triple whammy (link.springer.com)
- Variation in benzodiazepine and antipsychotic use in people aged 65 years and over in New Zealand (pubmed.ncbi.nlm.nih.gov)
- A whole of population retrospective observational study on the rates of polypharmacy in New Zealand 2014 to 2018 Polypharmacy in New Zealand: What is the current status? (onlinelibrary.wiley.com)
- Preventing acute kidney injury: assessing awareness to temporarily discontinue 'at-risk' medicines during acute illness in a New Zealand cohort (pubmed.ncbi.nlm.nih.gov)
Consumer resources
Atlas reports
Rural-urban variation
This short report summarises rural–urban differences in polypharmacy atlas indicators across New Zealand.
Method
Data for this Atlas domain was drawn from the Pharmaceutical Collection, which contains claim and payment information from community pharmacists for subsidised dispensing.
The data presented does not allow for analysis of patients’ condition or the effectiveness of dose provided. This means it was not possible to assess the appropriateness or otherwise of prescribing. Instead, proxy markers were employed, beginning with a simple count of the number of long-term medicines taken by older people. Unsubsidised or over-the-counter medicines are not included. Data also does not indicate whether people took the medicine.
References
- Polypharmacy and medicines optimisation (kingsfund.org.uk)
- Medication safety in polypharmacy: technical report (who.int)
- RACGP aged care clinical guide (Silver Book) (racgp.org.au)
- NSAIDS and acute kidney injury (medsafe.govt.nz)
- Psychotropic Drug-Induced Falls in Older People (link.springer.com)
- Psychotropic medication use and future unexplained and injurious falls and fracture amongst community-dwelling older people: data from TILDA (pubmed.ncbi.nlm.nih.gov)
- Australian and New Zealand Hip Fracture Registry Annual Report 2024 (anzhfr.org)